
- HYGEIA
- Services




Neuromas are benign tumours that enlarge slowly, compressing first their nerve of origin and, later, adjacent nerves and brain. This enlargement must be stopped before it does irreversible damage.
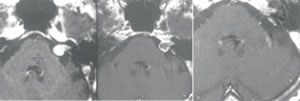
Figure showing the response of an acoustic neuroma to radiosurgery over two years
The available treatments are open surgical removal and Gamma Knife radiosurgery. Gamma Knife offers an equally good control of the tumour and avoids most of the risks and complications of open surgery. For this reason it is generally recognized as the treatment of choice for any neuroma less than 3cm diameter. The comparison of Gamma Knife with traditional microsurgery is summarized in the table:
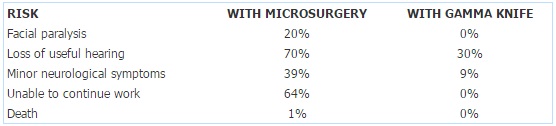
The success rate of Gamma Knife in controlling the growth of neuromas is 96%, equal to surgery where death and recurrence together equal 4%. However radiosurgery works slowly over several months as shown in the figure below. Sometimes the tumour may swell slightly before it begins to shrink. Follow up with MRI therefore continues for at least two years. Gamma Knife is not suitable for very large tumours causing symptoms of pressure on the brain stem. These must be removed surgically. It may be safer to perform a partial removal and treat any residual fragment by Gamma Knife. This has a greater chance of avoiding complications than with total removal.
Due to great improvements in surgical technique and the introduction of cranial nerve monitoring, microsurgeons have reduced the mortality and morbidity of acoustic neuroma surgery. Samii (1) has reported 97% tumour control with 93% normal facial movement (Grade I-II) and 47% hearing preservation. At the time of publication (1997) this was equal to the results from the ‘B’ series Gamma Knife (90% facial function and 50% hearing preservation). However, unfortunately, not all patients can be operated by a Samii. Average results, including those from the American Acoustic Neuroma Registry, are 90% tumour control (10% recurrence or death), 80% adequate facial nerve function and 6-30% hearing preservation (2,3). In addition there is 1% or more mortality even in centers of excellence (2).
At the same time the results from using highly conformal and selective, multiple isodose Gamma knife treatment with the ‘C’ series machine have improved. The results reported contemporaneously (4,5), using a marginal dose of 12Gy, are of 100% normal facial function and 59-70% hearing preservation (see graph below) together with 96% control of tumour growth.Except for having 0% mortality, the Gamma Knife treatment also has a much lower incidence than microsurgery of the minor complications and disabilities that are usually not discussed but are common after open operation (6). For example, minor neurological or functional deterioration (GK 9%, microsurgery 39%), hospital stay (GK 3 days, microsurgery 23 days), time away from work (GK 7 days, microsurgery 130 days), proportion keeping the same job (GK 100%, microsurgery 56%) (5).
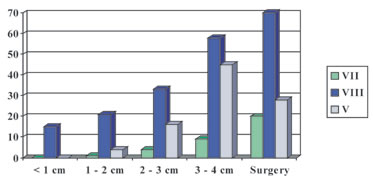
Risk of a difunction of local cranial nerves after Gamma Knife treatment of the acoustic neuromas of different size compared to open microsurgeryREFERENCES
- Samii M, Matthies C. Management of 1000 vestibular schwannomas (acoustic neuromas): surgical management and results with an emphasis on complications and how to avoid them. Neurosurgery 1997; 40: 11-23.
- Pollock BE, Lunsford LD, Noren G. Vestibular schwannoma management in the next century: a radiosurgical perspective. Neurosurgery 2000; 43: 475-483.
- Torrens M, Maw R, Coakham H, Butler S. Facial and acoustic nerve preservation during excision of extracanalicular acoustic neuromas using the suboccipital approach. Br J Neurosurg 1994; 8: 655-665.
- Iwai Y, Yamaka K, Shiotani M, Vyama T. Radiosurgery for acoustic neuromas: results of low dose treatment. Neurosurgery 2003; 53: 282-287.
- Regis J, Pellet W, Delsanti C et al. Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas. J Neurosurg 2002; 97: 1091-1100.
- © 2007-2024 HYGEIA S.M.S.A.

- Services