
- HYGEIA
- Services




What is osteoporosis?
Bone is a living tissue, but as we get older it isn’t able to renew itself as well so it starts to weaken. This happens to everybody to some extent, though it’s only called osteoporosis when the bones become quite fragile. There are usually no symptoms, and it’s often only discovered when you break a bone in a minor accident or fall.
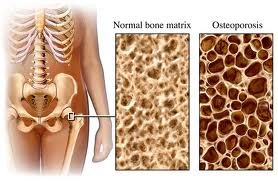
The word “osteoporosis” literally means porous (spongy) bone. It causes your bones to become fragile, so they break more easily.Bone is made up of minerals, mainly calcium salts, bound together by strong collagen fibers. Our bones have a thick, hard outer shell (called the cortex, cortical bone, or sometimes compact bone) which is easily seen on X-rays. Inside this, there’s softer, spongy bone (or trabecular bone) which has a honeycomb-like structure.
Bone is a living, active tissue that’s constantly renewing itself. Old bone tissue is broken down by cells called osteoclasts and replaced by new bone material produced by cells called osteoblasts.The balance between the breakdown of old bone and the formation of new bone changes at different stages of our lives.
- In childhood, new bone is formed very rapidly. This allows our bones to grow in length.
- Later, in our teens and early 20s, the bones stop growing in length, but continue to grow in density and strength. Bone density reaches its peak by our mid to late-20s.
- After this, new bone continues to be produced at about the same rate as older bone is broken down. This means that the adult skeleton is completely renewed over a period of 7-10 years.
- Eventually, bone starts to be broken down more quickly than it’s replaced, so our bones gradually begin to lose their density. This phase usually starts at about the age of 40 and continues for the rest of our lives.
We all have some degree of bone loss as we get older, but the term “osteoporosis” is used only when the bones become significantly more fragile. When bone is affected by osteoporosis, the holes in the spongy bone become larger, which is why the bone is more prone to fracture.
Who gets osteoporosis?
Osteoporosis mainly affects women, particularly after the menopause, but it can also affect men.
The risk of osteoporosis increases with age. Anyone can get osteoporosis but women are about 4 times more likely than men to develop it. There are 2 main reasons for this:
• The process of bone loss speeds up for several years after the menopause, when the ovaries stop producing estrogen.
• Men generally reach a higher level of bone density before the process of bone loss begins. Bone loss still occurs in men, but it may never reach a point where the bone is significantly weakened.
A number of other risk factors can affect our individual chances of developing osteoporosis and of breaking a bone in a relatively minor accident.What causes osteoporosis?
You’re at greater risk of developing osteoporosis if:
- you’ve needed steroid treatment for more than 3 months
- you have a family history of osteoporosis
- you don’t get much exercise
- you smoke or drink heavily
If you’re a woman, your risk may be increased if you’ve been through the menopause, especially if it was before the age of 45.
Risk factors include:
Cortisone
Taking cortisone can affect the production of bone, partly by reducing the amount of calcium absorbed from the gut and increasing calcium loss through your kidneys.
Estrogen deficiency – Women who’ve had an early menopause (before the age of 45) or a hysterectomy where one or both ovaries have been removed are at greater risk. Removal of the ovaries only (ovariectomy or oophorectomy) is relatively rare, but is also associated with an increased risk of osteoporosis.Lack of exercise
Moderate exercise encourages bone development. Anyone who doesn’t exercise, or who has an illness or disability that makes exercise difficult, will be more prone to losing calcium from the bones and more likely to be diagnosed with osteoporosis. Women who exercise so intensively that their periods stop are also at a higher risk.
Poor diet – People whose diet doesn’t include enough calcium or vitamin D or who are significantly underweight are at greater risk of osteoporosis.Heavy smoking
Tobacco lowers the estrogen level in women and may cause early menopause. In men, smoking lowers testosterone activity and this can also weaken the bones.
Heavy drinking – Drinking a lot of alcohol reduces the ability of your body’s cells to make bone. It also increases the risk of breaking a bone as a result of a fall.Family history
Osteoporosis runs in families. This is probably because there are inherited factors that affect the development of bone. If a close relative has suffered a fracture linked to osteoporosis, then your own risk of a fracture is likely to be greater than normal. We don’t yet know if a genetic defect causes osteoporosis, although we do know that people with a very rare genetic disorder called osteogenesis imperfecta are more likely to develop osteoporosis.
What treatments are there for osteoporosis?
Your doctor may recommend one or more of the following treatments:
- calcium and vitamin D
- bisphosphonates (e.g. alendronate, risedronate)
- strontium ranelate
- teriparatide
- denosumab
- raloxifene, bazedoxifene (SERMS)
- hormone replacement therapy (HRT)
- calcitonin
If you’re diagnosed with osteoporosis following a low-impact fracture, the first priority will be to treat the fracture. The next step is to begin treatment to reduce your risk of further fractures.
Treatment of fractures
Unless you have a vertebral fracture (a fracture of the backbone) you’ll usually need to see a specialist for an orthopedic assessment. They can decide whether the fracture needs to be fixed.
You may need pain relief, especially if you have a vertebral fracture. This can include:- painkillers, such as paracetamol, codeine and occasionally morphine
- non-steroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, naproxen, etc
- calcitonin and teriparatide, which has been shown to reduce pain from fractures of the pelvis and vertebrae
Prevention of fractures
Self-help measures, such as eating a healthy diet and exercising, can help to reduce your risk of fractures, but a number of specific treatments are also available. Your treatment will depend on your individual circumstances, and you should discuss this with your doctor. Types of treatment include:
- calcium and vitamin D
- bisphosphonates (e.g. alendronate, risedronate, ibandronate, etidronate, zolendronate)
- strontium ranelate
- teriparatide
- raloxifene, bazedoxifene (SERMS)
- denosumab
- calcitonin
- hormone replacement therapy (HRT)
Self-help and daily living
Try the following tips to help ease your symptoms: Plenty of calcium, vitamin D, proteins and other micro- or macronutrients (e.g. magnesium, sodium, fluoride, vitamins C, A and K) as part of a well-balanced diet.
Other ways to protect yourself against osteoporosis include:- Exercise – especially activities that involve running or jogging
- Stop smoking
- Don’t drink too much alcohol
Exercise
Exercise is important for your general health, but keeping physically active will also help you to:
- strengthen your bones
- keep your muscle strength
- improve your co-ordination (which reduces your risk of falling and of fractures)
Weight-bearing exercises (any activity that involves walking or running) are better for bone strength than non-weight-bearing exercises, such as swimming and cycling.
Diet and nutrition
You need to make sure that your diet has the right amount of calcium in it. Sources of calcium include:
- milk
- cheese (e.g. gruyere, emmental, parmesan)
- yogurt
- certain types of fish which are eaten with the bones (e.g. mackerel, herring, sardine)
- leafy green vegetables (e.g. cabbage, spinach, broccoli)
- watercress
- beans, chick peas, lentils
- some nuts (hazelnuts, almonds), seeds and dried fruits (e.g. dried figs)
Calcium is often added to white bread and some soya milks.
If you’re on drug treatment for osteoporosis, you may benefit from 1,000 -1,200 mg of calcium a day. A pint of milk and a reasonable amount of other foods that contain calcium should be enough.
Vitamin D is sometimes called the “sunshine vitamin” because it’s produced by your body when your skin is exposed to sunlight. It’s also found in some foods, especially oily fish, and is added to some soya milks and vegetable margarines. You may need to take a daily supplement containing vitamin D, especially if you’re over 60. Usually 10-20 micrograms (μg) daily is enough.What else might help?
Smoking can affect your hormones and so may increase your risk of osteoporosis. We strongly recommend you stop smoking – especially if you’re at risk for other reasons.
If you drink a lot of alcohol it can affect the production of new bone, so you should keep to the maximum amounts suggested by the government:- 2-3 units a day for women
- 3-4 units for men
- © 2007-2024 HYGEIA S.M.S.A.

- Services