



- HYGEIA
- Virtual tour
- Services
- Maternity Clinic
- Maternity Clinic Medical Services
- Paediatric Clinic
- Paediatric Clinic Medical Services



- HYGEIA
HYGEIA
- Virtual tour
Virtual tour
- Services
Services
- Maternity Clinic
Maternity Clinic
- Maternity Clinic Medical Services
Maternity Clinic Medical Services
Meningiomas are tumours, usually benign, which arise from the covering membrane of the brain. If they are on the convexity surface they can usually be removed surgically.
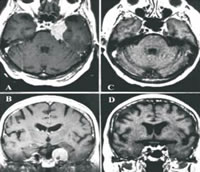
A cavernous sinus meningioma before (upper) and two years after (lower) Gamma Knife treatment
If they are under the brain on the skull base they may wrap themselves around nerves and arteries making complete removal dangerous or impossible. In such cases it has been shown that Gamma Knife treatment can control up to 99% of smaller tumours. When the tumour is very large, that part which can be removed safely should be excised and any remainder around arteries and nerves should be treated with the Gamma Knife. In this way effective combined treatment can be curative with minimal risk.
The mortality and morbidity of total surgical removal of meningiomas of the skull base and venous sinuses is still unacceptably high. Many surgeons elect to perform a subtotal removal in which case recurrence during the patient’s lifetime is at least 55%.
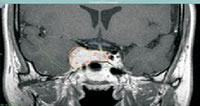
Illustration for the dose plan for an infiltrating meningioma of the cavernous sinus showing conformal treatment (yellow line). Even the lowest doses (10Gy, Green Line) can be designed to avoid structures such as the optic chiasm (Blue line)
Gamma Knife therapy has been shown to control 96-99% of meningiomas less than 3cm diameter, with two thirds of the tumours becoming smaller (1,2). Average morbidity (usually transient cranial nerve palsies) is 2%. This control is maintained over the long term. A ten year follow up study, which would have used the inferior, less conformal techniques of the ‘U’ and ‘B’ series gamma knives, showed 93.1% tumour control (3).
It is no longer acceptable to damage the patient by attempting complete removal of meningiomas. Elective surgical policy should be primary gamma knife treatment of tumours less than 3cm diameter (except those on the convexity dural surface) and partial removal followed by Gamma Knife treatment for larger tumours. If the tumour is very close to the optic nerve then a cushion of fat, Teflon or other material should be inserted to create a space between the tumour and the nerve. This allows safer and more effective radiosurgery later (the same applies to pituitary tumours). During a recent EANS debate the notable experts Al Mefty, Samii and Dolenc all agreed with this strategy. Al Mefty suggested waiting until the residual tumour actually shows signs of growth since, as noted above, the tumour may remain dormant.
REFERENCES
- Kondziolka D, Lunsford LD, Flickinger JC. Current concepts in gamma knife radiosurgery. Neurosurg Quart 1993; 3: 253-271.
- Prasad D, Phillips CD, Steiner M, Steiner L. Outcomes for gamma knife surgery in cavernous sinus meningiomas. Proc 8th Leksell Gamma Knife Society Meeting 1997, p22.
- Lunsford LD. Long term outcomes after gamma knife radiosurgery for cavernous sinus meningiomas. Proc 11th Leksell Gamma Knife Society Meeting 2002, p73.

- Services
- Virtual tour
- HYGEIA
- Paediatric Clinic
- Services
- Virtual tour